Quick Hits
Summary
- Antidepressant discontinuation syndrome is characterized by the FINISH mnemonic, with the “core” symptoms being “ISH”: dizziness (imbalance), brain zaps (sensory disturbances), irritability/agitation and anxiety/nervousness (hyperarousal)
- They happen after abrupt cessation or marked reduction in dose in a chronic (>1 mo) antidepressant, onset within 2-4 days of stopping and can last weeks up to months, or even years in the case of protracted withdrawal
- Similar to opioid/benzo withdrawal (physical dependence) but without drug craving reinforcing effects (psychological dependence)
- TCA and SNRI discontinuation can also overlap with cholinergic and noradrenergic rebound respectively
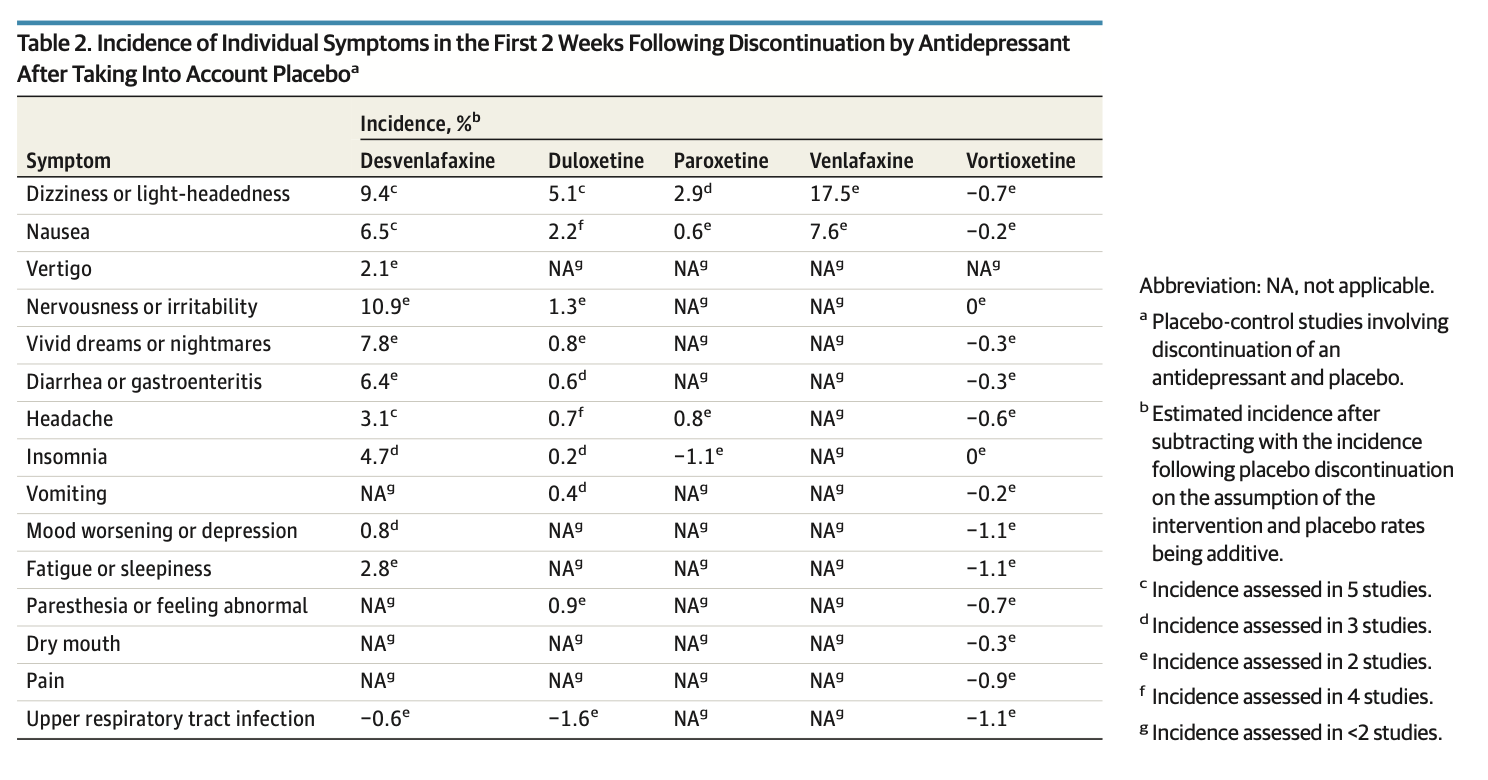
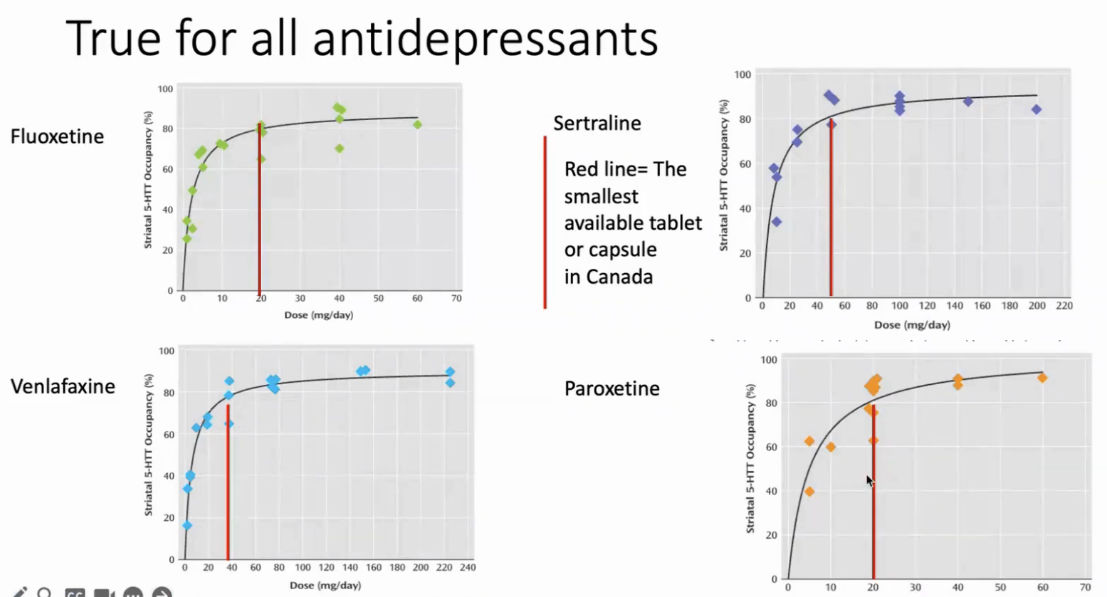
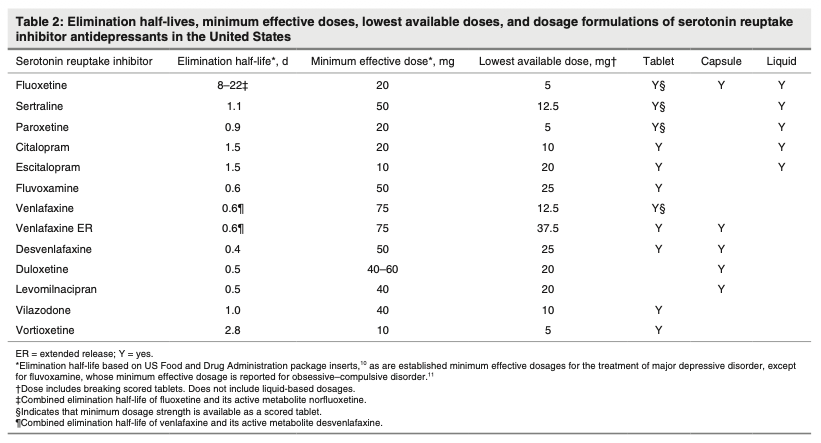
- Biggest risk factor is half life: paroxetine, venlafaxine, duloxetine worst; fluoxetine best by long shot due to active metabolite norfluoxetine leading to effective half-life on the order of weeks
- Slow, gradual tapering over weeks to months (ideally using a hyperbolic or proportionate dose reduction approach) combined with psychological support is the most effective strategy for minimizing discontinuation syndrome. Similar principles to benzos, opioids, Z-drugs, gabapentinoids, antipsychotics, mood stabilizers, beta blockers, PPIs.
- Fluoxetine substitution protocol (2025): gradual taper to lowest tolerable dose that is commercially available (ie by 50% q4wks), then start Prozac 5mg/day for 4 weeks, then taper original SRI off and wait 4 weeks, then taper off the fluoxetine to once weekly
Recognize and Assess
Definitions
- “Antidepressant discontinuation syndrome is a set of symptoms that can occur after an abrupt cessation (or marked reduction in dose) of an antidepressant medication that was taken continuously for at least 1 month.” [DSM-V]
- “To qualify as antidepressant discontinuation syndrome, the symptoms should not have been present before the antidepressant dosage was reduced and are not better explained by another mental disorder (e.g., manic or hypomanic episode, substance intoxication, substance withdrawal, somatic symptom disorder).” [DSM-V]
- “Discontinuation symptoms may occur following treatment with tricyclic antidepressants (e.g., imipramine, amitriptyline, desipramine), serotonin reuptake inhibitors (e.g., fluoxetine, paroxetine, sertraline), and monoamine oxidase inhibitors (e.g., phenelzine, selegiline, pargyline).” [DSM-V]
Onset and Duration
- “Symptoms generally begin within 2–4 days and typically include specific sensory, somatic, and cognitive-emotional manifestations.” [DSM-V]
- “For some people, antidepressant discontinuation symptoms can be mild and transient, but in other cases, symptoms can be more severe and last longer” [UK NICE Guidelines]
- Duration: symptoms are usually self-limited, typically lasting about a week, but can persist for weeks to months or even years in some individuals, particularly after abrupt discontinuation of short half-life agents.
- “The antidepressant discontinuation syndrome is based solely on pharmacological factors and is not related to the reinforcing effects of an antidepressant.” [DSM-V]
Symptoms
- “Vague and variable” [DSM-V]
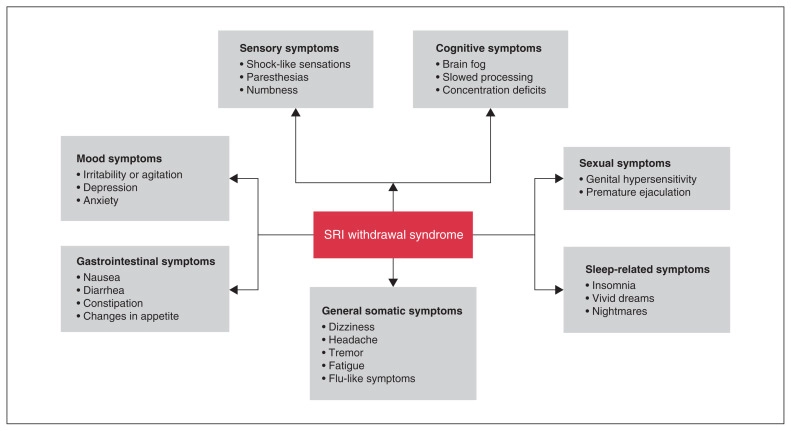
- The FINISH mnemonic captures the typical symptom cluster: Flu-like symptoms, Insomnia, Nausea, Imbalance, Sensory disturbances, Hyperarousal.
- FLU-LIKE: Fatigue, lethargy, myalgias, chills, headache. May overlap with actual viral illness; fatigue was NOT significantly associated with discontinuation vs. placebo [Kalfa et al, 2025]
- INSOMNIA: Sleep disturbance, vivid/disturbing dreams, increased dreaming. Most commonly rated “severe”
- NAUSEA: Nausea, vomiting, diarrhea, decreased appetite. Nausea was the 2nd most common symptom
- IMBALANCE: Dizziness, vertigo, lightheadedness, ataxia/unsteady gait. Dizziness was the single most common symptom, likely related to serotonin’s effects on the vestibular system
- SENSORY DISTURBANCES: “Brain zaps”/electric shock sensations (often with moving eyes), paresthesias, tinnitus, visual disturbances. Frequently reported sensory and somatic symptoms include flashes of lights, “electric shock” sensations, nausea, and hyperresponsivity to noises or lights. Nonspecific anxiety and feelings of dread may also be reported.” [DSM-V]
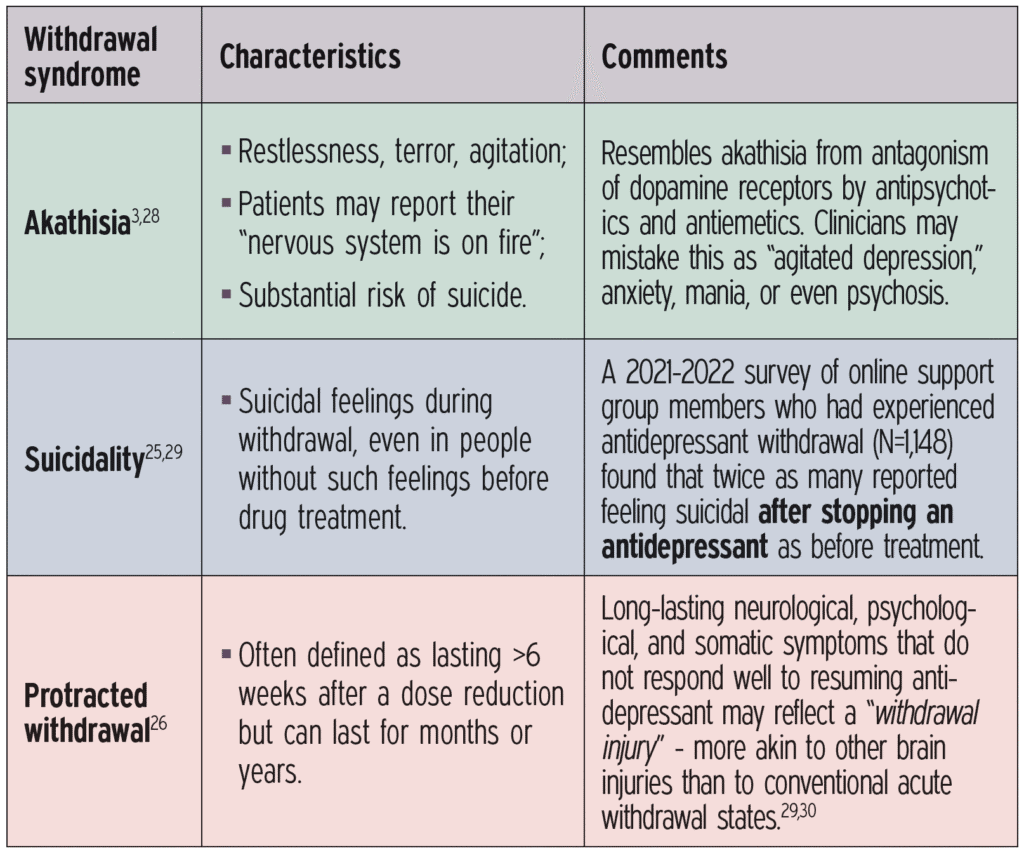
- HYPERAROUSAL: Anxiety/nervousness, irritability, agitation, aggression, crying spells, mood swings, tachycardia (sometimes arrhythmias), akathisia, even suicidality (Mark Horowitz). Nervousness and anxiety symptoms may be mistaken for reemergent anxiety disorder.
- A 2023 survey of 344 patients found that nearly all (97.7%) reported worsening of at least one of four “core” symptoms: dizziness, brain zaps, irritability/agitation, or anxiety/nervousness — suggesting these four symptoms may be more specific to SRI withdrawal than the broader FINISH categories (ie “ISH” > “FIN”)
- Increase in suicide attempts in the 2 weeks after stopping an antidepressant (Valuck et al, 2009)
- Akathisia “can’t keep still”, pacing, sense of terror, nervous system feels like it is on fire. Most recognized as a side effect of long-term antipsychotics but can occur in withdrawal from antidepressants and other psychotropics as well. Often misdiagnosed as agitated depression or mania.
DDx: relapse of anxiety or depression?
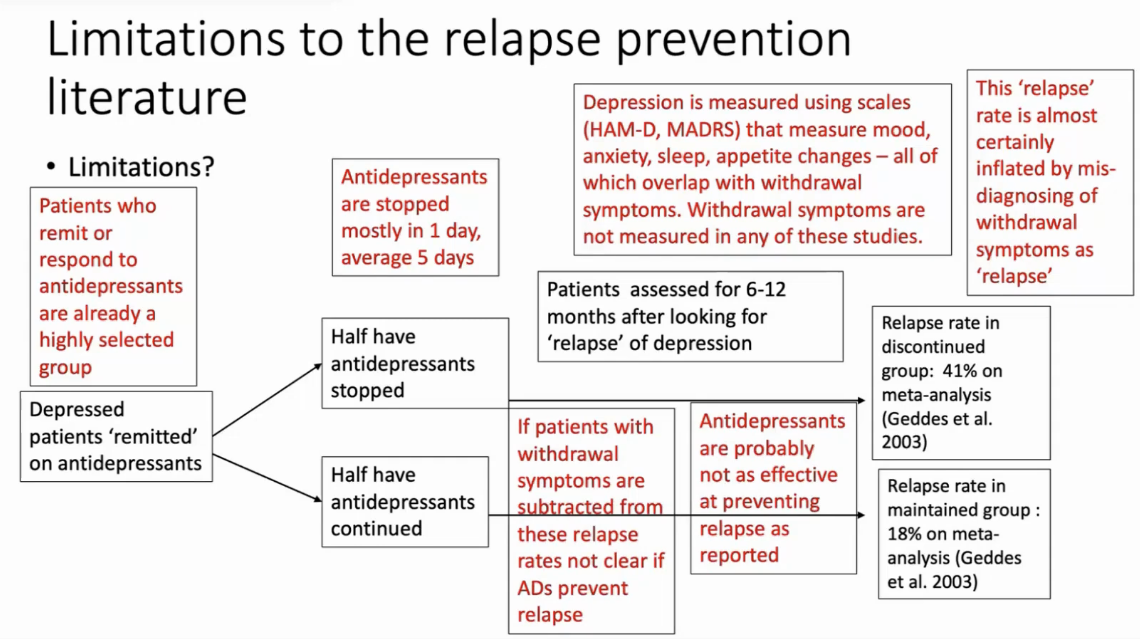
- Withdrawal effects are misdiagnosed as relapse of depression or anxiety
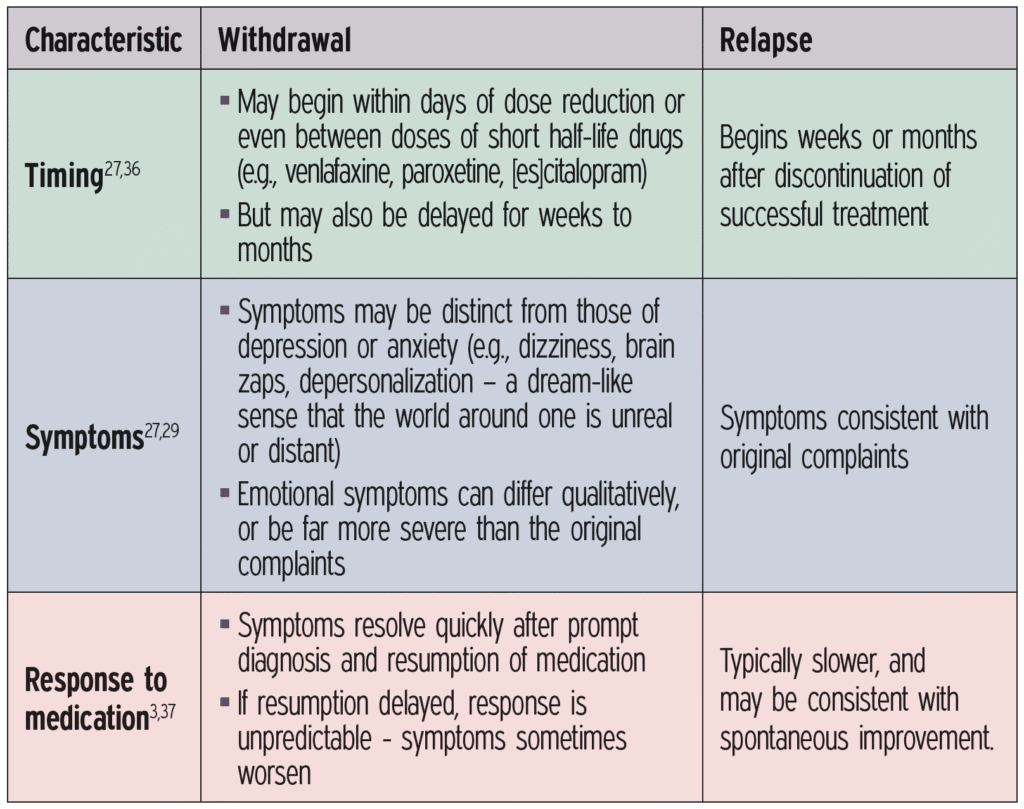
- Clues that it is more likely withdrawal
- withdrawal can be quick onset, but also can be delayed
- specific symptoms (dizziness, brain zaps) not present before, or no new stressors like grief
- often quick resolution on re-instatement of antidepressant (hours to days)
- An important finding from the 2025 JAMA Psychiatry meta-analysis: discontinuation was NOT associated with worsening depressive symptoms in the first 2 weeks, even in patients with MDD. This suggests that early mood worsening after stopping is more likely withdrawal-related anxiety/hyperarousal, while later-onset depressive symptoms (beyond 2 weeks) more likely represent true relapse.
- “Also, in the case of stimulant augmentation of an antidepressant, abrupt cessation may result in stimulant withdrawal symptoms rather than the antidepressant discontinuation syndrome” [DSM-V]
Anticipate
Risk factors
- Half-life: shorter t½ → more abrupt drop in receptor occupancy → higher risk (paroxetine, venlafaxine, desvenlafaxine, duloxetine)
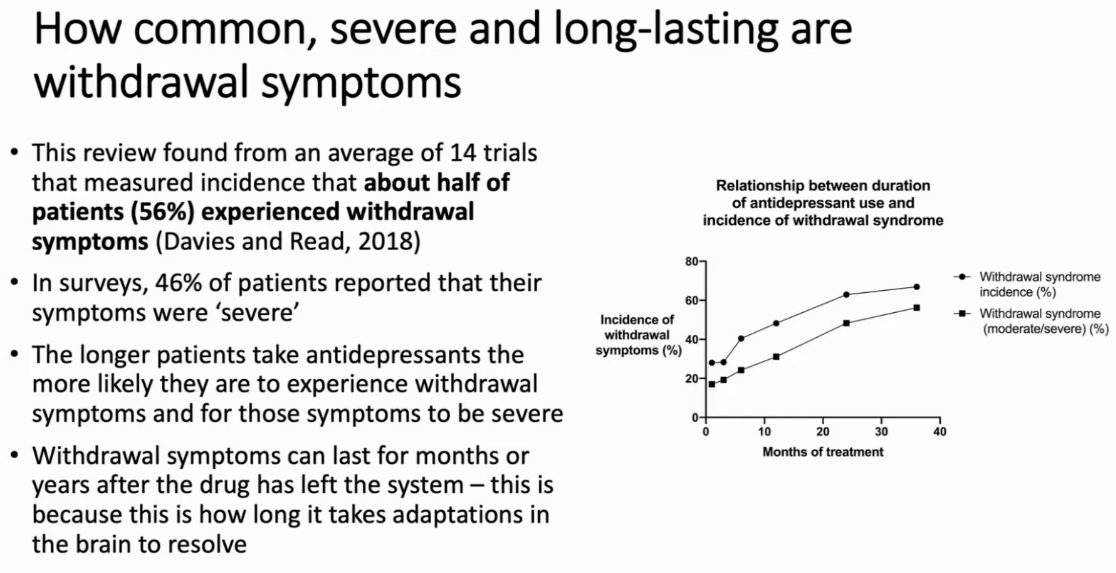
- Duration of use: longer treatment may produce greater neuroadaptation, though the 2025 Kalfas meta-analysis did not find a significant association in RCT data (possibly due to shorter treatment durations in trials vs. real-world practice)
- Dose: weak association with higher doses, with possible ceiling effects reflecting receptor occupancy saturation
- CYP metabolizer status: rapid/ultrarapid metabolizers may experience faster drug clearance and greater symptom risk
- Individual genetic susceptibility: not well characterized but likely contributes to the wide interindividual variability
- Cholinergic Rebound (TCAs): loss of muscarinic anticholinergic blockade in the setting of supersensitized receptors produces a state of cholinergic overdrive, manifesting as GI cramping, nausea, diaphoresis, and headache.
- Noradrenergic Rebound (SNRIs, TCAs): additional adrenergic rebound may contribute, may explain symptoms such as agitation, anxiety, and autonomic instability.
Half-life
Below is a comprehensive table of antidepressant half-lives compiled from FDA drug labels and recent pharmacokinetic literature, organized by class. The half-life is the single most important pharmacokinetic parameter influencing discontinuation syndrome risk, with shorter half-life agents (paroxetine, venlafaxine) carrying the highest risk. [OpenEvidence: various sources including the Lancet, NEJM, Seminars in Dialysis, Clinical Pharmacokinetics]
Worst for stopping: paroxetine, venlafaxine, desvenlafaxine, duloxetine [Horowitz] Better: bupropion (more similar to an amphetamine), agamelatine [Horowitz]
| Drug | Class | Parent t½ (hours) | Active Metabolite (t½) | Discontinuation Risk |
|---|---|---|---|---|
| SSRIs | ||||
| Fluoxetine | SSRI | 24–72 (acute); 96–144 (chronic) | Norfluoxetine (96–384 h) | Low |
| Citalopram | SSRI | 33–37 | Desmethylcitalopram (weakly active) | Moderate |
| Escitalopram | SSRI | 27–32 | S-DCT (weakly active) | Moderate |
| Sertraline | SSRI | 22–36 | Desmethylsertraline (62–104 h, weakly active) | Moderate |
| Fluvoxamine | SSRI | 15–22 | None significant | Moderate |
| Paroxetine | SSRI | 21 (nonlinear ↑ with dose) | None | High |
| SNRIs | ||||
| Milnacipran | SNRI | 6–8 | None significant | Low |
| Levomilnacipran | SNRI | 12 | None significant | Low |
| Duloxetine | SNRI | 10–12 | None significant | Moderate |
| Desvenlafaxine | SNRI | 10 | None significant | High |
| Venlafaxine | SNRI | 5 | O-desmethylvenlafaxine (12 h) | High |
| Atypical / Other | ||||
| Vortioxetine | Multimodal | 57–66 | None significant | Moderate |
| Mirtazapine | NaSSA | 20–40 | Desmethylmirtazapine (weakly active) | Unclear |
| Bupropion | NDRI | 12–21 | Hydroxybupropion (20–37 h) | Unclear |
| Vilazodone | SPARI | 25 | None significant | — |
| Trazodone | SARI | 5–9 | mCPP (weakly active) | — |
| Agomelatine | MT₁/MT₂ agonist | 1–2 | None significant | No risk |
| TCAs | ||||
| Clomipramine | TCA | 22–84 | Desmethylclomipramine | High |
| Amitriptyline | TCA | 31–46 | Nortriptyline (18–93 h) | High |
| Nortriptyline | TCA | 18–93 | 10-hydroxynortriptyline | High |
| Desipramine | TCA | 14–62 | 2-hydroxydesipramine | High |
| Imipramine | TCA | 9–24 | Desipramine (14–62 h) | High |
| Doxepin | TCA | 8–24 | Desmethyldoxepin (9–33 h) | High |
| MAOIs | ||||
| Tranylcypromine | MAOI | 2–3 (irreversible MAO inhibition lasts ~2 weeks) | — | Very high |
| Phenelzine | MAOI | 2 (irreversible MAO inhibition lasts ~2 weeks) | — | Very high |
Management
Taper
Historical guidance
- “Most international depression guidelines acknowledge and support tapering of antidepressants when discontinuing them, but there remains variability in duration and types of withdrawal symptoms among antidepressants.” [Kalfa et al, 2025]
- CANMAT 2019: “we recommend slowly tapering the dose over several weeks or months”, but no details on how to do this. This is based on one study that showed abruptly stopping caused too severe withdrawal effects and that 4 weeks was considered a reasonable time by the committee (expert consensus).
- Most common approach “over the past 2 decades” internationally: reduce dose by half for 2-4 weeks, reduce dose to quarter for 2-4 weeks (often by alternating half a tablet every second day)
- But most people can’t come off using this regimen, and leaves “at least 60% of patients trapped on their medications” [Mark Horowitz]. People turning to peer support websites like “Surviving Antidepressants” or “The Withdrawal Project”, which recommend weaning at 10% of the most recent dose ever month (hyperbolic-like)
DSM-V
- “Symptoms are alleviated by restarting the same medication or starting a different medication that has a similar mechanism of action—for example, discontinuation symptoms after withdrawal from a serotonin-norepinephrine reuptake inhibitor may be alleviated by starting a tricyclic antidepressant.” [DSM-V]
- “Because longitudinal studies are lacking, little is known about the clinical course of antidepressant discontinuation syndrome. Symptoms appear to abate over time with very gradual dosage reductions. After an episode, some individuals may prefer to resume medication indefinitely if tolerated.” [DSM-V]
Current evidence
[OpenEvidence]
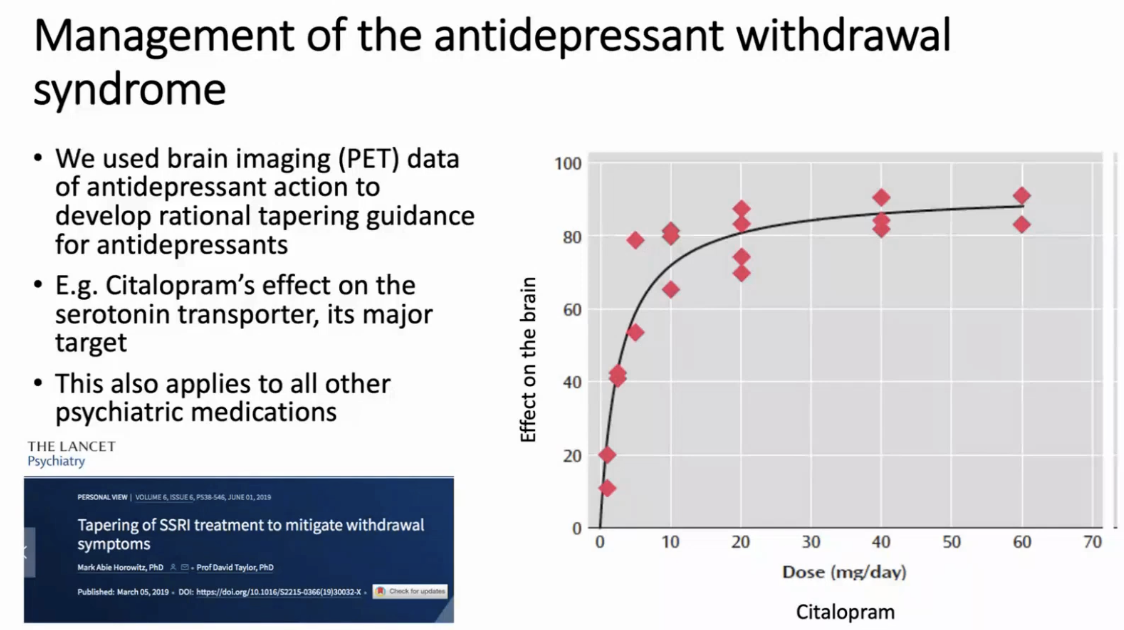
- The best current evidence supports slow, gradual tapering over weeks to months — ideally using a hyperbolic dose-reduction approach — combined with psychological support as the most effective strategy for minimizing discontinuation syndrome and preventing relapse.
- Short tapers are inadequate: A critical finding across the literature is that the traditional 2–4 week tapers recommended by older guidelines show minimal benefit over abrupt discontinuation and are often not tolerated [Horowitz & Taylor, 2019]. In contrast, tapering over several months dramatically reduces withdrawal incidence: paroxetine tapered over an average of ~39 weeks had only a 6.1% incidence of withdrawal syndrome vs. 78.2% with abrupt discontinuation. [2021 Cochrane review]
Hyperbolic tapering
[Horowitz & Taylor, 2019]
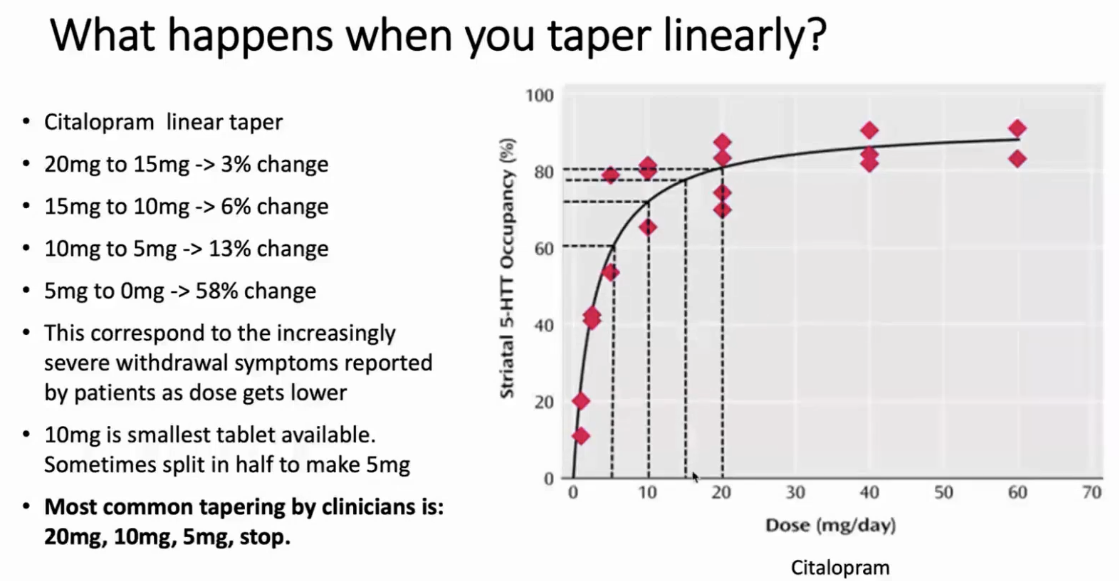
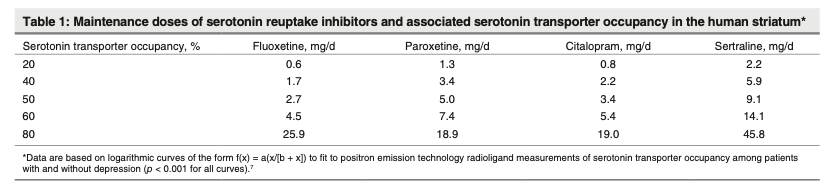
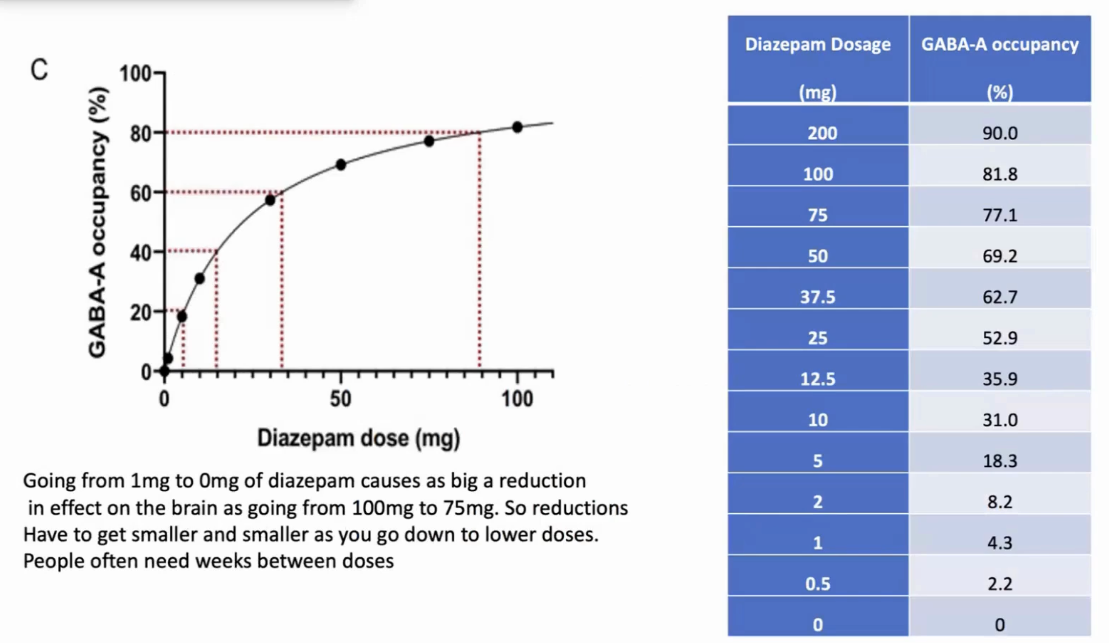
- Reducing from 20 mg → 10 mg of an SSRI produces a relatively small drop in SERT occupancy (e.g., ~80% → ~65%)
- Reducing from 5 mg → 2.5 mg produces a proportionally much larger drop in receptor occupancy
- Reducing from 2.5 mg → 0 mg produces the largest relative change
Therefore, equal absolute dose reductions (e.g., cutting by 5 mg each step) produce unequal pharmacological effects — with the final steps being the most destabilizing. Hyperbolic tapering addresses this by making progressively smaller dose reductions as the dose gets lower, achieving approximately equal reductions in SERT occupancy at each step. In practice, this means reducing by a fixed proportion of the current dose (e.g., ~10% of the current dose every 2–4 weeks), which requires reaching doses well below the minimum therapeutic dose — sometimes as low as 1/40th of the standard dose — before stopping.
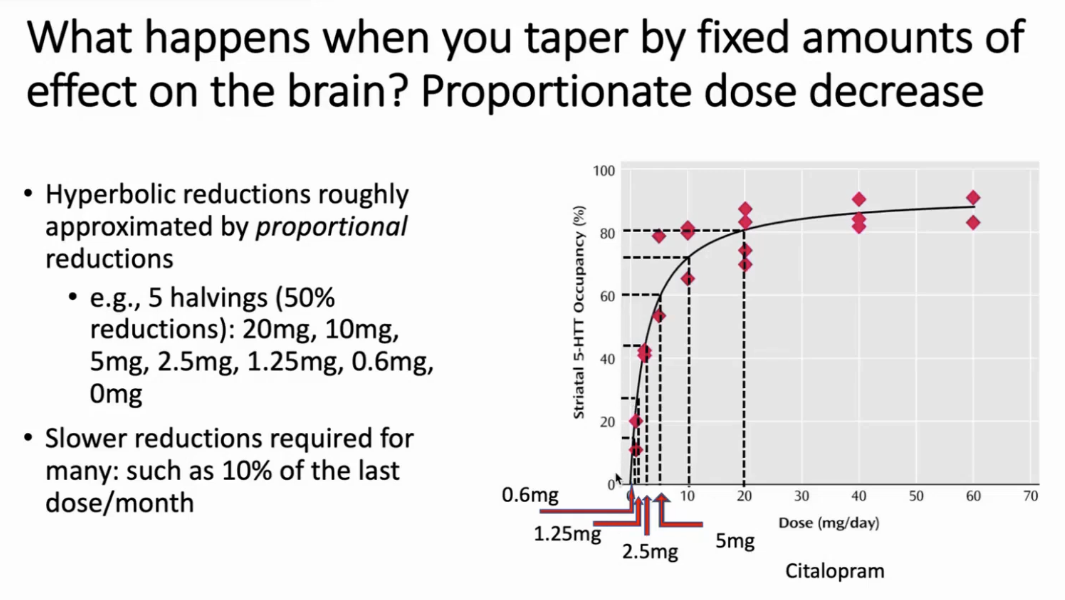
It’s never true that when you are on a “small dose” you can just stop it. [Horowitz]
In one study of 895 patients where ⅔ had been unable to stop antidepressants in usual quick linear taper, 71% were able to stop with a hyperbolic taper over months (Groot and van Os, 2018)
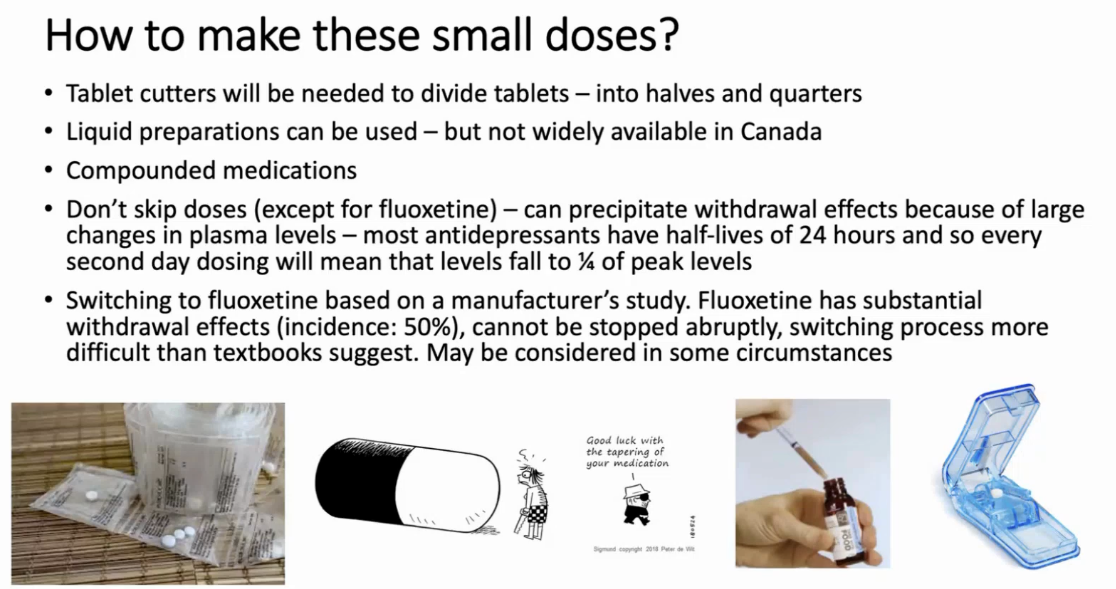
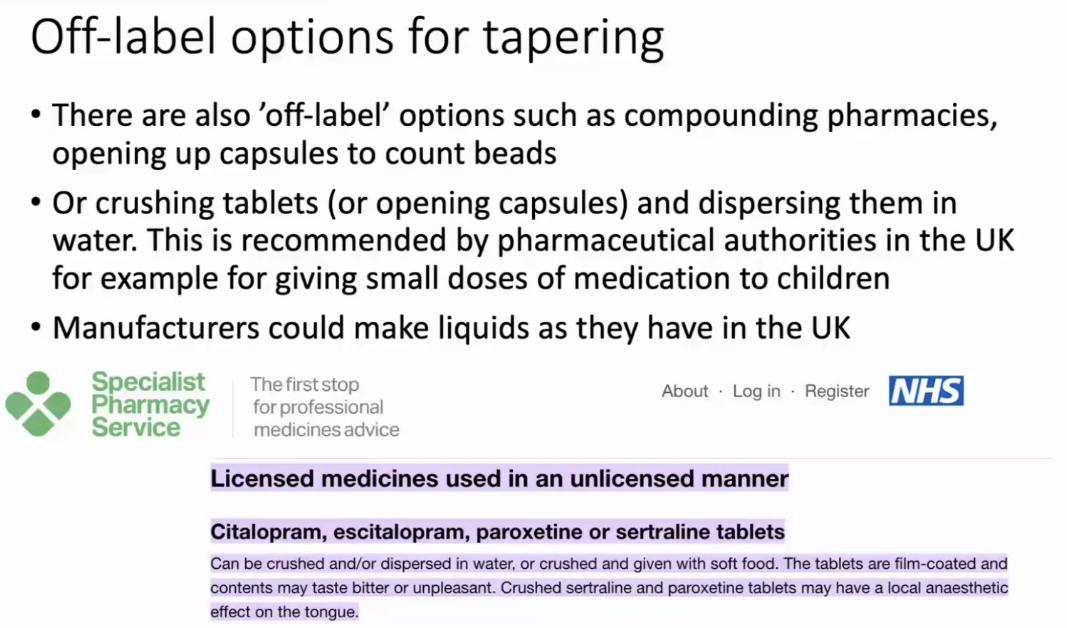
“Cheat code”: any immediate release tablet, put in 300mL of water, stir with spoon x 15s. If you remove 30mL per month it’s 10% deduction.
Practical Tapering Protocols
The AAFP (2023) recommends two reasonable strategies:
- Standard taper: ~25% dose reduction every 4 weeks
- Faster taper: ~12.5% dose reduction every 2 weeks
A gradual taper has been shown to result in as few as 5% of patients experiencing discontinuation symptoms.
For high-risk drugs (paroxetine, venlafaxine, desvenlafaxine), longer tapers are essential — NICE and the UK Royal College of Psychiatrists now recommend months of tapering, particularly for short half-life agents. Tapering strips (used in Dutch studies) that allow dose reductions to very small fractions of the minimum therapeutic dose achieved successful discontinuation in 71% of 895 participants (97% of whom had prior withdrawal), with 68% remaining off antidepressants at 1–5 year follow-up.
Fluoxetine Bridging Strategy
For patients struggling to discontinue short half-life SRIs (paroxetine, venlafaxine), switching to fluoxetine is a well-recognized strategy. Fluoxetine’s long elimination half-life (~4–6 days for parent compound, ~9–19 days for norfluoxetine) provides a built-in “self-taper” that minimizes the abrupt drop in SERT occupancy. That being said, Mark Horowitz does not believe this as it was extrapolated from a manufacturer’s study that only looked for withdrawal symptoms for 1 week, but fluoxetine effects can be delayed and as hard to come off as any other antidepressant, just that the studies didn’t look far enough…
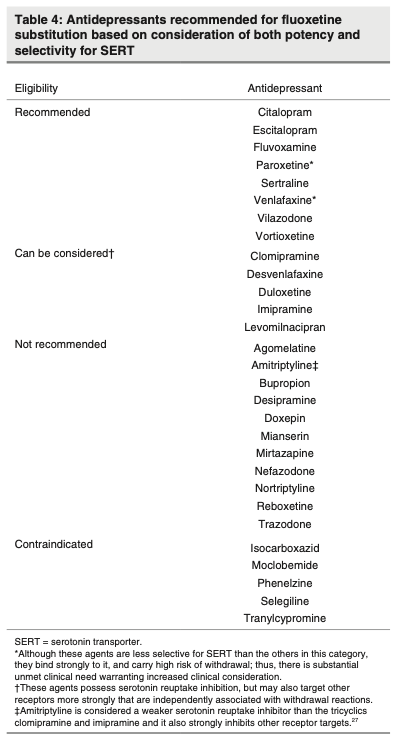
A 2025 standardized fluoxetine substitution protocol [Shapiro & Cohrs, 2025] has been proposed to facilitate this approach for patients who cannot access compounding, liquid formulations, or bead-counting methods. Not recommended for atypical antidepressants or TCAs though like bupropion, mirtazapine, trazodone, or doxepin.
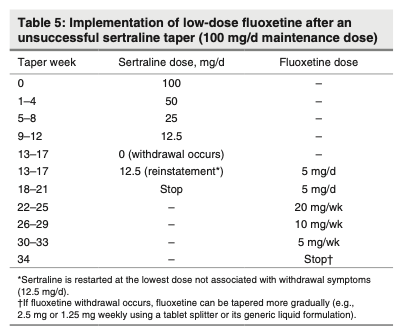
4 step process:
- Step 1: Taper the original SRI to the lowest tolerable dose that is commercially available, as gradually as practicable (e.g., initially, 50% dosage reduction every 4 weeks). Tapering the SRI as much as possible before introducing fluoxetine may reduce the risk of serotonergic and other adverse effects associated with SRI co-treatment. If intolerable withdrawal symptoms occur, the previous dose should be reinstated, followed by a more gradual dosage reduction (e.g., 25% dosage reduction every 4 weeks or the smallest dosage reductions allowed by the standard dosage formulary), if possible, before moving to the next step.
- Step 2: Add fluoxetine 5 mg/d and maintain combination treatment for 4 weeks. Based on estimates modelled from PET radioligand data, 4 weeks of fluoxetine treatment at 5 mg/d results in an average 60% SERT occupancy, which should mitigate withdrawal effects when the original SRI is tapered and discontinued. Significantly higher doses of fluoxetine (e.g., 15–20 mg) may unnecessarily increase the risk of adverse effects without commensurate benefit. At 4 weeks, blood fluoxetine concentrations are likely to be at steady state, whereas norfluoxetine levels may modestly increase for an additional 6 weeks in some individuals.
- Step 3: Taper the original SRI using commercially available dosages. We suggest an initial taper schedule of 50% dose reductions every 4 weeks to the lowest available conventional dosage before discontinuing the SRI. If intolerable withdrawal symptoms occur at this pace, the lowest tolerable dose should be reinstated, followed by a more gradual dosage reduction (e.g., 25% reduction every 4 weeks), if commercially available.
- Step 4: Taper and discontinue fluoxetine. After the patient has fully discontinued their original SRI, we recommend monitoring for at least 4 weeks to assess for withdrawal symptoms longitudinally and to ensure stability on fluoxetine before tapering. After this period, fluoxetine should be switched from 5 mg/d to a a once-weekly dosing phase, with reductions occurring every 4 weeks.

Slow Tapering + Psychological Support: The Best Combined Strategy
The most recent and comprehensive evidence comes from the Zaccoletti et al. (2026) Lancet Psychiatry network meta-analysis — the first to directly compare all major deprescribing strategies head-to-head. Key findings:
- Slow tapering (>4 weeks) combined with psychological support (CBT or MBCT) prevented relapse to a similar extent as antidepressant continuation and clearly outperformed abrupt discontinuation or fast tapering
- Discontinuation with psychological support achieved successful discontinuation rates of 40–75%
- The ASCP (2026) expert consensus further supports individualized deprescribing, favoring discontinuation when mechanisms are duplicative or adequate trials show ≤25% improvement, while recommending indefinite maintenance after ≥3 lifetime depressive episodes
Managing Breakthrough Symptoms
If intolerable symptoms emerge during tapering:
- Reinstate the prior dose — symptoms typically resolve within 24 hours
- Then resume tapering at an even slower rate
- Additional symptomatic management (e.g., short-term benzodiazepines for severe anxiety, antihistamines for insomnia) may be used adjunctively
Summary
A major caveat: despite growing consensus, the optimal tapering protocol remains formally undefined — most recommendations are based on pharmacological reasoning, observational data, and expert consensus rather than large head-to-head RCTs of specific tapering schedules.
| Principle | Recommendation |
|---|---|
| Taper duration | Minimum 4 weeks; months preferred for high-risk drugs |
| Taper method | Hyperbolic (proportional dose reductions, smaller steps at lower doses) |
| Dose reduction rate | ~25% of current dose every 4 weeks, or ~10% every 2–4 weeks |
| Final dose before stopping | Well below minimum therapeutic dose (potentially 1/40th) |
| Psychological support | CBT or MBCT during taper reduces relapse to levels comparable to continuation |
| High-risk agents (paroxetine, venlafaxine) | Consider fluoxetine bridging or liquid formulations for micro-tapering |
| Breakthrough symptoms | Reinstate prior dose → resume slower taper |
Antidotes
- TCA withdrawal symptoms often respond to anticholinergic agents (atropine, benztropine)
Lost PO Access
- ideally cross taper before this happens
- otherwise just treat symptomatically with sedation PRN
Deeper Dive
History
“The prevalence of antidepressant discontinuation syndrome is unknown but is thought to vary according to the dosage prior to discontinuation, the half-life and receptor-binding affinity of the medication, and possibly the individual’s genetically influenced rate of metabolism for this medication.” [DSM-V]
- Official guidance prior to 2019 [Mark Horowitz]
- CANMAT: “withdrawal effects are mild to moderate in severity and resolve within a few weeks”. The 2024 update of Canadian depression guidelines (CANMAT) recognized that “up to 50% of patients may experience discontinuation symptoms when stopping long-term use of antidepressants, especially with abrupt stopping.”
- Influenced by papers produced by drug companies in the 1990s, which focused on people who had used antidepressants for 8-12 weeks. Then at a consensus panel organised by an antidepressant manufacturer, the euphemism ‘discontinuation symptoms’ was coined, and numerous papers with the description ‘brief and mild’ were attributed to clinicians.
- But we know that the longer you use them, the more you adapt to them, the more severe and common and long lasting the withdrawal syndrome can be, so this guidance can be very misleading. Most people who use it in real life are using it for years and decades. “kind of like a car company testing a car crash at 5 km/h and saying it is safe at 60km/h”
Incidence
- “The incidence of this syndrome depends on the dosage and half-life of the medication being taken, as well as the rate at which the medication is tapered. Short-acting medications that are stopped abruptly rather than tapered gradually may pose the greatest risk. The short-acting selective serotonin reuptake inhibitor (SSRI) paroxetine is the agent most commonly associated with discontinuation symptoms, but such symptoms occur for all types of antidepressants.” [DSM-V]
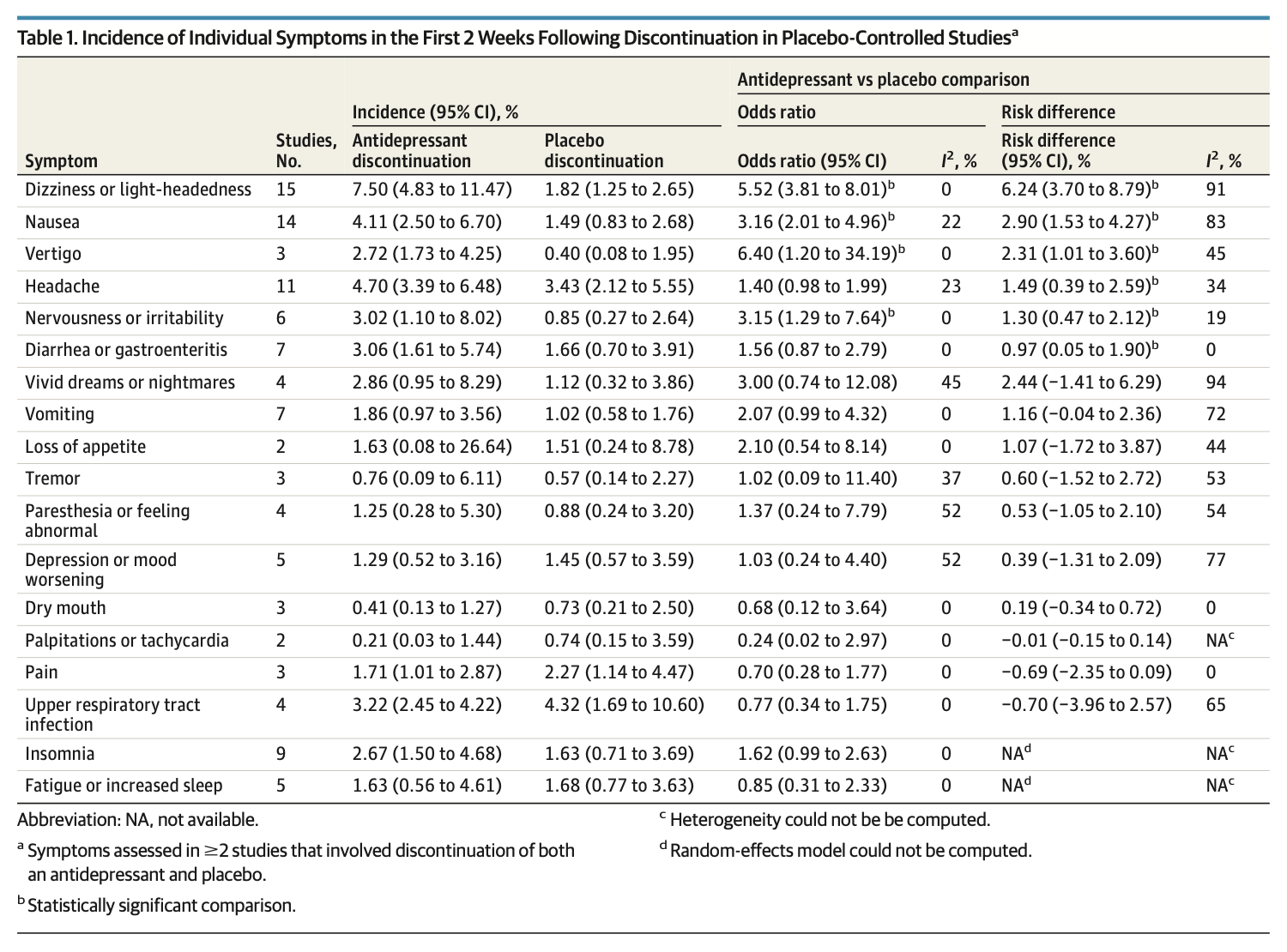
- “This systematic review and meta-analysis of 49 randomized clinical trials found that on average, participants who stopped antidepressants experienced 1 more discontinuation symptom compared to those who discontinued placebo or continued antidepressants. The most common symptom in the first 2 weeks following antidepressant discontinuation was dizziness [followed by nausea], and discontinuation of antidepressants was not associated with depressive symptoms.” [Kalfa et al, 2025]
- “In conclusion, data from RCTs suggest that on average, those who discontinue antidepressants experience 1 more discontinuation symptom compared to placebo or continuation of antidepressants, which is below the threshold for clinically important discontinuation syndrome. Mood change was not seen in antidepressant discontinuation. While acknowledging that discontinuation symptoms exist, results of this systematic review and meta-analysis suggest that the rates are lower than those reported in prior reviews. The need for prolonged tapering regimens is open to question, with concerns previously noted, in addition to possible nocebo effects. This, therefore, requires careful examination through methodologically rigorous, placebo-controlled RCTs in real-world settings.” [Kalfa et al, 2025]
- The Discontinuation-Emergent Signs and Symptoms (DESS) checklist is the standard research tool, and a score of ≥4 new symptoms has been used as the cutoff for clinically significant discontinuation syndrome.
Pathophysiology
[OpenEvidence] The pathophysiology of antidepressant discontinuation syndrome remains incompletely understood, but the best current evidence points to several converging neurobiological mechanisms, with the most robust recent data coming from the 2024 Collins et al. preclinical study and the 2024 Sharp & Collins mechanistic review.
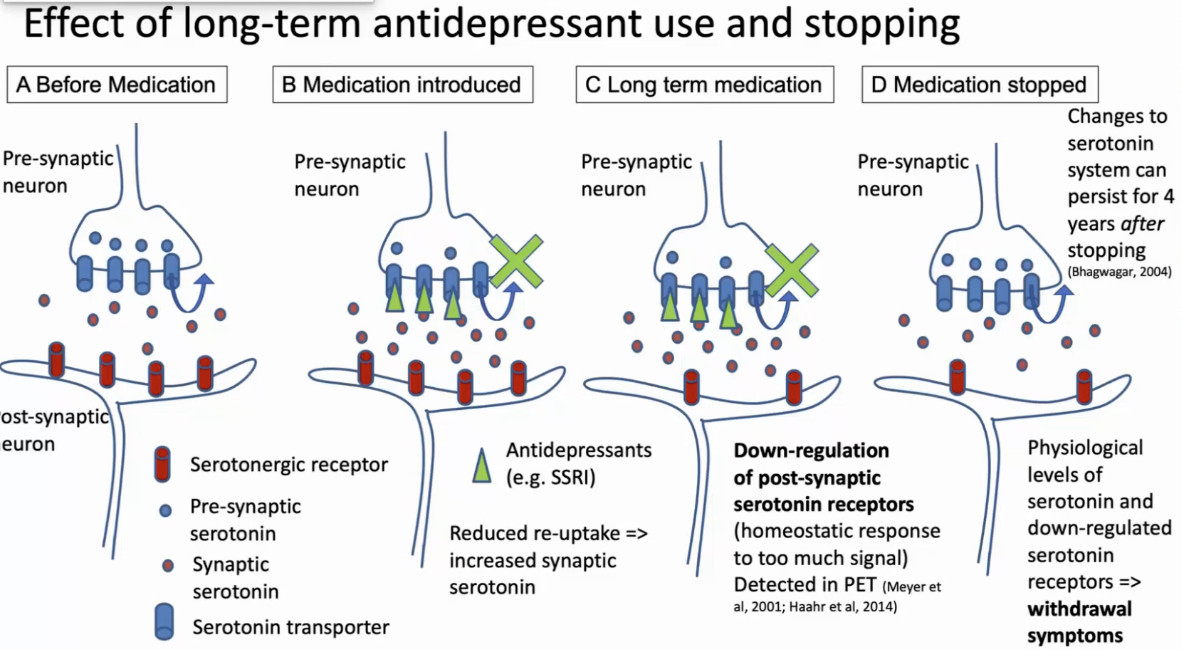
- The Central Mechanism: Homeostatic Neuroadaptation and Rebound
- Daily receptor activation triggers downstream neuroadaptive changes (receptor sensitivity, density, neurotransmitter availability) to establish a new physiological set point, analogous to benzos or opioids but without drug craving or reinforcing effects
- Serotonergic Rebound Hyperexcitability (SSRIs/SNRIs)
- Mouse model of paroxetine discontinuation (Collins et al, 2024) demonstrated a rebound activation of 5-HT neurons leading to a hyperactive serotonergic system
- The Serotonin Receptor Downregulation Hypothesis
- Chronic SSRI use leads to postsynaptic 5-HT receptor downregulation (previous hypothesis from Schatzberg et al, 1997). Contradicted by above, both reduced and increased 5-HT release and neuronal firing suggesting a dysregulated rather than simply deficient serotonergic state
- Hyperbolic Dose–Occupancy Relationship and SERT Occupancy
- From PET imaging: relationship between antidepressant dose and serotonin transporter (SERT) occupancy follows a hyperbolic (Michaelis-Menten) curve: occupancy rises steeply at low doses and plateaus at ~80% at the minimum therapeutic dose. Horowitz & Taylor (2019, Lancet Psychiatry) argued that this means linear dose reductions produce disproportionately large drops in SERT occupancy at lower doses, potentially explaining why standard short tapers (2–4 weeks) often fail to prevent symptoms.
- However, the 2025 Kalfas et al. JAMA Psychiatry meta-analysis noted that this SERT occupancy model “does not explain individual variation or high incidence of discontinuation symptoms with drugs like paroxetine,” and that abrupt discontinuation of desvenlafaxine was not associated with notably greater symptoms than tapered discontinuation — raising questions about the clinical applicability of the hyperbolic tapering rationale.
- Cholinergic Rebound (TCAs)
- For tricyclic antidepressants, a distinct mechanism operates. TCAs are potent muscarinic receptor antagonists, and chronic use leads to upregulation and supersensitization of muscarinic cholinergic receptors. Upon discontinuation, the loss of anticholinergic blockade in the setting of supersensitized receptors produces a state of cholinergic overdrive, manifesting as GI cramping, nausea, diaphoresis, and headache. This “cholinergic overdrive hypothesis” was demonstrated experimentally by Dilsaver et al. (1987), who showed that chronic amitriptyline supersensitized central muscarinic mechanisms in rats. TCA withdrawal symptoms often respond to anticholinergic agents (atropine, benztropine), supporting this mechanism.
- Noradrenergic Rebound (SNRIs, TCAs)
- For drugs with norepinephrine reuptake inhibition (venlafaxine, duloxetine, TCAs), an additional adrenergic rebound component may contribute, analogous to beta-blocker withdrawal. This is less well characterized than the serotonergic and cholinergic mechanisms but may explain symptoms such as agitation, anxiety, and autonomic instability.
- Symptom-Specific Mechanisms
- Dizziness/vertigo (the most common placebo-adjusted symptom, RD 6.24%): likely related to serotonin’s role in the vestibular system, where 5-HT modulates vestibular nucleus activity
- “Brain zaps”/electric shock sensations: the mechanism remains unknown, though these are highly characteristic of SRI withdrawal and were identified as one of four “core” symptoms by Shapiro et al. (2023). Hypotheses include aberrant serotonergic modulation of sensory processing or transient cortical hyperexcitability, but no definitive neurobiological substrate has been identified
- Sleep disturbance/vivid dreaming: may relate to serotonin’s role in REM sleep suppression; withdrawal of serotonergic tone leads to REM rebound
- Risk Modifiers
- The degree of neuroadaptation — and therefore discontinuation risk — is influenced by:
- Half-life: shorter t½ → more abrupt drop in receptor occupancy → higher risk (paroxetine, venlafaxine)
- Duration of use: longer treatment may produce greater neuroadaptation, though the 2025 Kalfas meta-analysis did not find a significant association in RCT data (possibly due to shorter treatment durations in trials vs. real-world practice)
- Dose: weak association with higher doses, with possible ceiling effects reflecting receptor occupancy saturation
- CYP metabolizer status: rapid/ultrarapid metabolizers may experience faster drug clearance and greater symptom risk
- Individual genetic susceptibility: not well characterized but likely contributes to the wide interindividual variability
The pathophysiology is best understood as a multi-system neuroadaptive rebound following removal of chronic pharmacological stimulation. For SSRIs/SNRIs, the most current evidence (Collins et al. 2024) points to rebound hyperexcitability of 5-HT neurons as a central mechanism, while the SERT occupancy model provides a pharmacokinetic framework for understanding dose-dependent risk. For TCAs, cholinergic receptor supersensitization and rebound overdrive is the dominant mechanism. Across all classes, the syndrome is pharmacologically driven and does not involve drug craving or addiction pathways.
Antidepressant MOAs
- TCAs have wide interindividual variability in half-life (e.g., nortriptyline 18–93 hours), making precise rank-ordering within the class approximate.
- Tricyclic antidepressants (TCAs) are named for their three-ring chemical structure — a central seven-membered ring fused to two flanking six-membered benzene rings, forming a characteristic tricyclic nucleus.
- For MAOIs, the parent compound half-lives are very short (2–3 hours), but the clinical effect persists for approximately 2 weeks due to irreversible enzyme inhibition — the pharmacodynamic duration, not the pharmacokinetic t½, drives the high discontinuation risk.
- Fluoxetine stands out across all classes: when accounting for its active metabolite norfluoxetine (t½ up to 16 days), the effective half-life is the longest of any antidepressant, which is why it carries the lowest discontinuation risk among SSRIs.-
- Trazodone is a SARI (serotonin antagonist and reuptake inhibitor), which blocks 5-HT₂A (and to a lesser extent 5-HT₂C) receptors with weak inhibition of serotonin reuptake (SERT blockade) compared to SSRIs or SNRIs. At low doses (trazodone 25–100 mg, commonly used for insomnia), the 5-HT₂A and histamine H₁ blockade predominate, producing sedation with minimal serotonin reuptake inhibition. This is why low-dose trazodone is widely used as a hypnotic rather than an antidepressant, while at higher doses (150–400 mg), SERT inhibition becomes more clinically relevant, contributing to antidepressant efficacy — though still weaker than SSRIs.
- This dual mechanism — blocking 5-HT₂A while only weakly inhibiting reuptake — is precisely why trazodone’s discontinuation syndrome risk is likely lower than that of SSRIs, as discussed in the prior response. The degree of SERT occupancy is the key driver of withdrawal neuroadaptation, and SARIs produce far less of it at typical doses.
- The Kalfas et al. 2025 JAMA Psychiatry meta-analysis did not include trazodone in its drug-specific subgroup analyses, meaning there were insufficient RCTs with DESS data to generate a trazodone-specific effect size.
- Vortioxetine is termed “multimodal” because it acts on multiple serotonergic targets simultaneously, rather than just blocking reuptake. It combines SERT inhibition (like an SSRI) with direct activity at several 5-HT receptor subtypes: 5-HT₃, 5-HT₇, and 5-HT₁D antagonism, 5-HT₁B partial agonism, and 5-HT₁A agonism. The net effect is enhanced serotonergic neurotransmission plus downstream increases in norepinephrine, dopamine, acetylcholine, histamine, and glutamate release — broader neurotransmitter modulation than SSRIs achieve. The 5-HT₃ antagonism is thought to be particularly important: it disinhibits glutamatergic pyramidal neurons (by reducing GABAergic interneuron activity), which may underlie vortioxetine’s pro-cognitive effects — a distinguishing clinical feature. At 5 mg, primarily SERT and 5-HT₃ receptors are occupied; at 20 mg, all targets reach functionally relevant occupancy.
- Mirtazapine (NaSSA — Noradrenergic and Specific Serotonergic Antidepressant) works through a fundamentally different mechanism than reuptake inhibitors — it does not block any monoamine transporter. Instead, it increases norepinephrine and serotonin release by blocking presynaptic α₂-adrenergic autoreceptors and heteroreceptors. Blocking α₂ autoreceptors on noradrenergic neurons removes the “brake” on norepinephrine release; blocking α₂ heteroreceptors on serotonergic neurons removes the noradrenergic inhibition of serotonin release. Simultaneously, mirtazapine blocks postsynaptic 5-HT₂A, 5-HT₂C, and 5-HT₃ receptors, which channels the increased serotonin toward 5-HT₁A-mediated neurotransmission (the pathway thought to mediate antidepressant effects) while avoiding the side effects associated with 5-HT₂ and 5-HT₃ stimulation (sexual dysfunction, nausea). Its potent histamine H₁ antagonism explains the prominent sedation and appetite stimulation, which paradoxically predominate at lower doses (15 mg) because at higher doses the increasing noradrenergic activity counteracts the antihistaminergic sedation.
- Bupropion is classified as a Norepinephrine-Dopamine Reuptake Inhibitor (NDRI). Its mechanism involves two key actions:
- Inhibition of norepinephrine (NE) and dopamine (DA) reuptake — blocking the transporters that clear these neurotransmitters from the synapse, thereby increasing their availability. Notably, bupropion is a relatively weak inhibitor of both transporters in vitro, and it has no clinically meaningful effect on serotonin reuptake. Because bupropion has no serotonergic activity, it avoids the typical SSRI/SNRI side effects — sexual dysfunction, weight gain, and GI disturbance — and carries an unclear/low discontinuation syndrome risk, as discussed in the earlier tables.
- Nicotinic acetylcholine receptor antagonism — bupropion blocks α3β4 nicotinic receptors, which is the basis for its FDA-approved use in smoking cessation.
- MT Agonists refers to melatonin receptor agonists, specifically drugs that activate MT₁ and MT₂ receptors in the suprachiasmatic nucleus (SCN) of the hypothalamus — the brain’s master circadian clock. The antidepressant action of agomelatine is thought to arise from the synergy between these two mechanisms — the melatonergic component restores circadian architecture and sleep quality, while the 5-HT₂C antagonism enhances catecholamine transmission. Importantly, agomelatine has no affinity for muscarinic, histaminergic, adrenergic, or dopaminergic receptors, and does not inhibit serotonin reuptake — which explains its favorable side effect profile (no sexual dysfunction, no weight gain, no GI effects) and its absence of discontinuation syndrome risk.
Protracted antidepressant withdrawal syndrome
- can last up to years
- looks like neurologic injury, trouble with balance, light sensitivity, bedbound, lost jobs. All the usual reasons when starting on them due to grief, work stress.
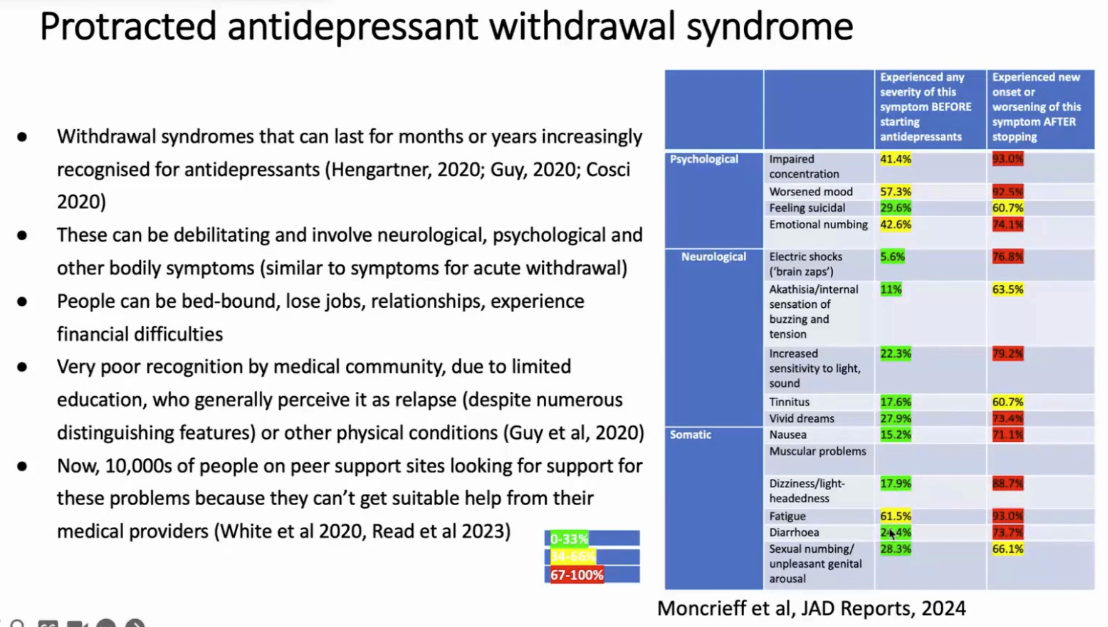
A lot of people get into worse symptoms after stopping antidepressants than prior to even starting it. Wished they never started.
Deprescribing
Why deprescribe?
- NNT for an antidepressant is 7, so 6/7 will have no response
- a lot of people using it longer than guidelines (6-12mo of therapy for anxiety/depression, many are on them for years or decades)
- Most are prescribed at a tough point in their lives with a stressor (divorce, job loss, physical health, death in family - with relapse unlikely)
- Alternative coping skills developed, people adapt
- Decreased side effects: sexual s/e, emotional numbing (>50%, even in health volunteers so not due to depression), fatigue/impaired memory/concentration, insomnia, worsened anxiety or depression (tardive dysphoria), weight gain (30% in longer term studies)
- health: increased risk of stroke, obesity, falls, CAD, osteoporosis, premature mortality, increased bleeding risk
- Many people believe antidepressants will correct a chemical imbalance (misleading)
- Pregnancy (increased risk of fetal abnormality by 2.5-3 fold in first trimester)
- Reduce pill burden, interactions with other meds
Other meds
Same hyperbolic curves in opioids, benzodiazepines, gabapentinoids, antipsychotics, mood stabilizers, stimulants (although generally easier to stop), even beta blockers, PPIs…
Informed consent
- Efficacy: NNT 7, so most people they won’t work
- 15% of people will have significant effect at 8 weeks, but they wear off over time
- S/e: emotional numbing, wt gain, cog impairment, insomnia, longer you use it the harder it is to stop, bleeding (esp if older)
- Alternatives: most people’s anxiety and mood issues stem from life circumstances. “What’s the cure for depression?“. People have relationship, financial, work problems, so it depends on the person. In the UK, there are 19 equally effective treatments for depression (2 are pharmacotherapy), exercise, therapy, mindfulness, problem solving therapy (single most cost effective treatment for severe depression)
- Name your 3 top problems, tell me the steps you will take to address the top one, come back in 2 weeks and tell me about barriers encounters or progress made.
- Speaks to the issues in people’s lives, not always easy to fix…
- Doing nothing: is a highly effective treatment for depression. Recovery rate for severe depression (enough to hospitalize) at 12 mo is 85% (better for mild depression). Internal documents from big pharma: we have a real problem with depression because the recovery rate is so good, there is no space for our treatments.
- “Wait and see approach”: ⅔ of people were remitted within 3 months with NO treatment; secondary care (psychiatry team)
- How to stop it: the longer you wait, the harder it’ll be, you might need a liquid, might take months or years, if you do it too quickly, can lead to severe problems coming off
- How do the drugs work? People are told it will fix a chemical imbalance in your brain. The problem is that it’s not true. The real answer is that we don’t know. All sorts of biological theories, but there is a very obvious reason: most people experience emotional numbing. This is very different than saying it will fix a chemical imbalance.
EOL
[Horowitz]
- <3 mo? What’s the point of starting antidepressants, no long term risks but you can make the last few months of her life even more horrible with these drugs
- Lost PO access: would try to give them via liquid to prevent withdrawal
Mea culpa
- https://blogs.bmj.com/bmj/2020/09/25/wendy-burn-medical-community-must-ensure-that-those-needing-support-to-come-off-anti-depressants-can-get-it/
- analogous to the opioid epidemic, doctors can be duped, are told that these risks are minimized
- “If I hadn’t come off of them myself, and developed akiathisia and suicidality that I’ve never had before, I never would have understood these things. A whole systems response is needed, to reduce prescribing, to help people stop quicker, set up clinics, pathways, provide liquids. Does require political will. Hope it doesn’t require lives lost or lawsuits from patients.” [Horowitz]
Gun to my head?
- would start Bupropion, with fluoxetine as a second choice. [Horowitz]
References
- Dr Mark Horowitz GHHN Rounds Apr 22/2026: https://www.youtube.com/watch?v=TXhlRSzzHqE&list=PLGZ546vp4yOpX34giR0K1brA2FO_xQ8i5&index=1
- JAMA 2025 Meta-Analysis: https://pubmed.ncbi.nlm.nih.gov/40632531/
- 2006 AAFP Article on Antidepressant Discontinuation Syndrome: https://www.aafp.org/pubs/afp/issues/2006/0801/p449.html
- 2019 Lancet Psychiatry Horowitz & Taylor: https://pubmed.ncbi.nlm.nih.gov/30850328/
- Cochrane review 2021: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD013495.pub2/full?__cf_chl_tk=yJiwJGhZbTuDSkb4B3_bwFymG7pzJW85lH25rfdjlDE-1778771272-1.0.1.1-lUYxCwZgQvUv5I3F.eYHpE4WcQ00951FJef97mvqO6o
- 2026 Zaccoletti study in Lancet Psychiatry: https://pubmed.ncbi.nlm.nih.gov/41386898/
- 2025 Shapiro and Cohrs fluoxetine substitution protocol: https://pubmed.ncbi.nlm.nih.gov/40610042/
- Royal College of Psychiatry in the UK: https://www.rcpsych.ac.uk/mental-health/treatments-and-wellbeing/stopping-antidepressants
- UBC Therapeutics Initiative: https://www.ti.ubc.ca/2025/06/18/156-antidepressant-withdrawal-syndrome-update/